Dermolipoma
Updated August 2025
Daniel B. Azzam, MD; Seanna R. Grob, MD
Establishing the diagnosis
Etiology
- Congenital; a choristoma (normal tissue in abnormal location)
- Embryologic ectopia of the ectoderm to conjunctiva, due to sequestration at the time of eyelid development (Kim, Am J Neuroradiol, 2011)
- Distinguished by abundant adipose tissue component and dense dermis-like fibroconnective tissue in deeper layers, covered by thick stratified squamous epithelium contiguous with the conjunctiva (Figure 1) (Shields, Curr Opin Ophthalmol, 2007)
- Pilosebaceous tissue may also be present
- Also referred to as lipodermoid
- Distinct but similar entity to limbal dermoid, which is a smaller inferotemporal corneal lesion comprised of squamous epithelium, hair follicles, and sebaceous glands
- Not to be confused with dermoid cyst – a superotemporal or superomedial orbital cyst of keratinized epithelium with dermal appendages and adnexal structures formed along a bony suture line
Figure 1. Dermolipoma. A. Epibulbar choristoma composed of dense collagenous stroma covered by conjunctiva-type epithelium. The stroma contains pilosebaceous units (black arrow), sweat glands (blue arrow) and abundant adipose tissue (asterisk). H&E original magnification x 20. B. Lobules of mature adipocytes separated by fibrous septa, intermixed with sweat glands (blue arrows). H&E original magnification x 200. C. Non-keratinized stratified squamous epithelium with PAS-positive goblet cells is covering the lesion. Periodic Acid-Schiff (PAS) original magnification x 100.
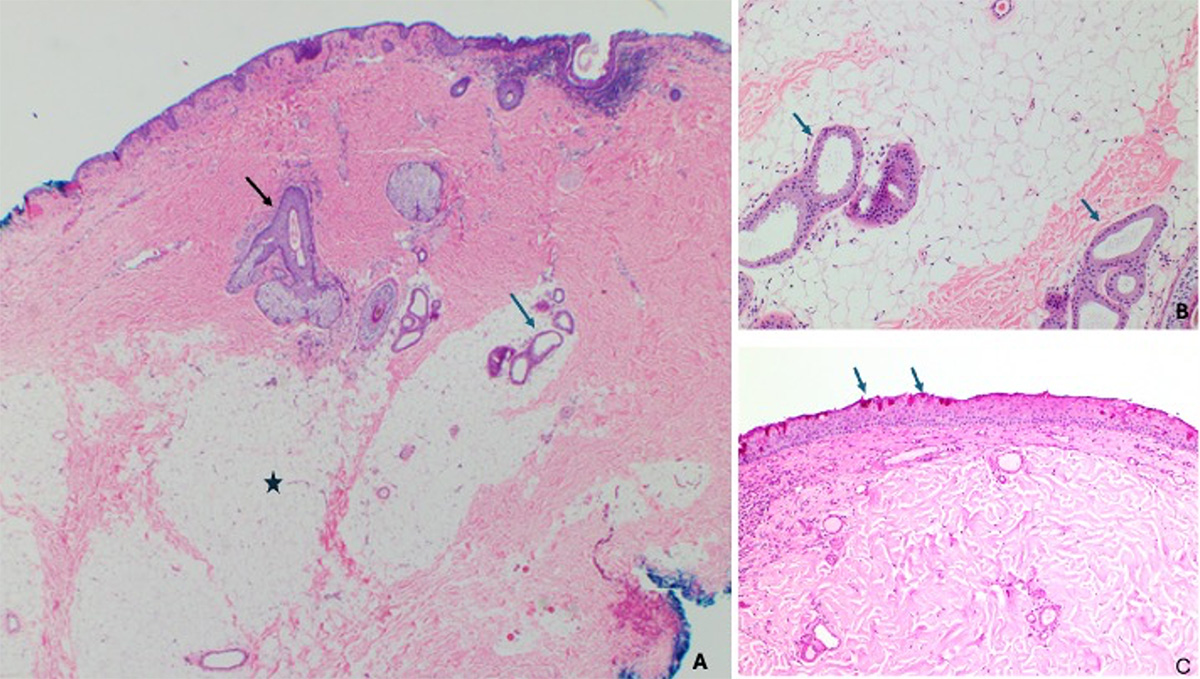
(Histopathological images made available by Dr. Maria Del Valle Estopinal, MD, Ophthalmic Pathology, Department of Ophthalmology, University of California, Irvine)
Figure 2. Dermolipoma. Hematoxylin and eosin-stained section shows a limbal mass resembling skin, lined by epidermis (keratinizing stratified squamous epithelium) and containing multiple hair follicles and adipose tissue.
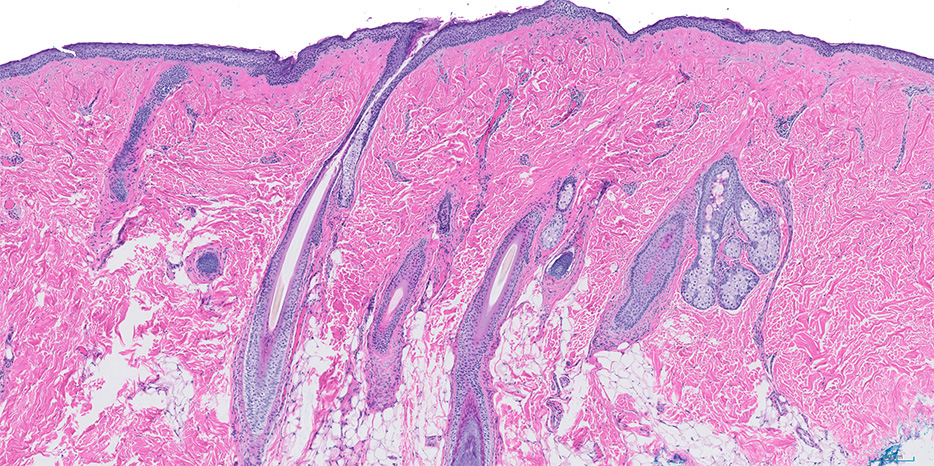
(Histopathologic image made available by Dr. Melike Pekmezci, Ophtahlmic Pathology, Department of Ophthalmology, University of California, San Francisco)
Epidemiology
- Dermolipoma is the second most common conjunctival tumor in children (5%) (Shields, Curr Opin Ophthalmol, 2007)
- Represents 3% of orbital lesions overall and is the most common lipocytic orbital lesion (Shields, Ophthalmology, 2004)
- Female predilection (Khong, Ophthalmology, 2013) and (McNab, Aust N Z J Ophthalmol, 1990)
- Age of presentation 20-22.5 years (Khong, Ophthalmology, 2013) and (McNab, Aust N Z J Ophthalmol, 1990)
History
- Classically presents as a beige-yellowish epibulbar mass located near the temporal fornix (Figure 3)
- Present at or near birth, but typically not detected until later in life during adolescence or early adulthood
- Often first noticed when lifting the eyelid to apply makeup or place contact lens
- Slowly grows as child ages
Figure 3. External photographs of two clinical images of dermolipomas

Clinical features
- Most common characteristics include growing chronic peribulbar lesion (73%), visible fine hairs (33%), ocular irritation (24%), lateral canthal widening (24%), episodic localized injection (12%), mucoid discharge (12%), and aberrant lacrimal gland ductules with opening onto skin (4%) (Vahdani, Ophthal Plast Reconstr Surg, 2021)
- Typically unilateral smooth and firm mass, firmly adherent to overlying conjunctiva
- Cannot be repositioned into the orbit, and does not increase in size with retropulsion as orbital fat prolapse would
- Not as freely mobile as orbital fat prolapse
- Can extend deep into orbit posteriorly and tends not to involve cornea anteriorly, though may disrupt the lateral canthus
- Mechanism of symptoms includes:
- Ocular surface irritation: pilosebaceous structure growth causing mechanical irritation or tear film disruption
- Disturbance of vision: ptosis or refractive error, though induced astigmatism is much less that that of limbal dermoids
- Associated abnormalities include features of Goldenhar syndrome, such as eyelid coloboma, limbal dermoid, pre-auricular skin tags, cervical vertebral anomalies, micrognathia, and strabismus related to Duane syndrom
Testing
Indications for imaging
- Typically easily diagnosed on clinical exam, but orbital imaging modalities may be utilized to confirm the diagnosis and for surgical planning
CT scan and MRI
- CT and MRI both can reliably distinguish dermolipoma from orbital fat prolapse and may delineate posterior extension
- CT should be avoided in children if possible, especially given the benign nature of dermolipoma
- Unilateral, crescent- or triangle-shaped fatty mass located at the temporal epibulbar area along lateral aspect of globe, anterior to insertion of lateral rectus muscle and medial to lacrimal gland (Figure 4) (Kim, Am J Neuroradiol, 2011)
- No radiographic evidence of connection to intraconal fat, in contrast to orbital fat prolapse
- Typically identical attenuation on CT or signal intensity on MRI compared to intraconal fat, though may display subtle soft tissue stranding on CT
Figure 4. Axial CT showing a dermolipoma on the left
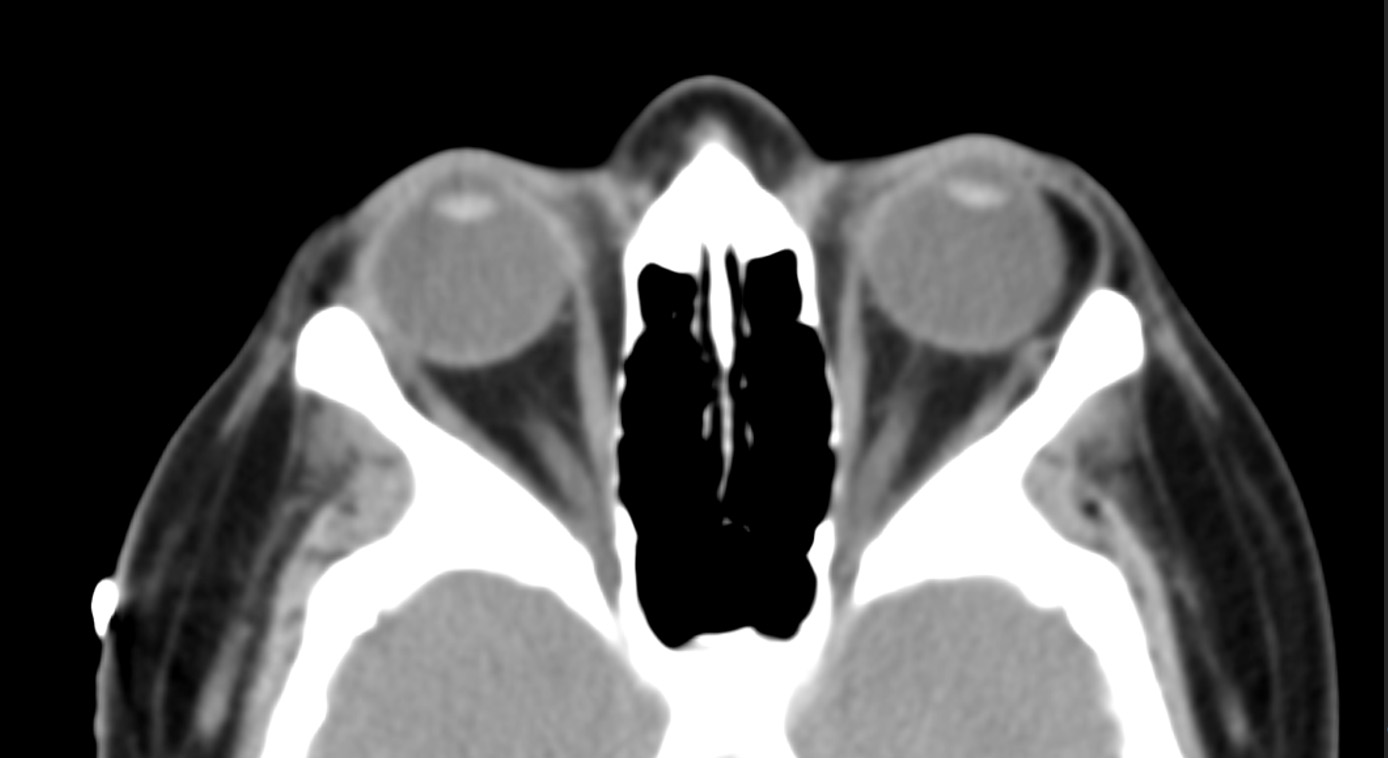
(Radiographic image made available by Dr. Edward Kuoy, Department of Radiology, University of California, Irvine)
Risk factors
- Most arise sporadically, though occasionally may be associated with a congenital syndrome:
- Oculo-Auriculo-Vertebral spectrum: Goldenhar syndrome, seen in 35% of dermolipoma cases, whereas conversely dermolipoma is seen in 32% of Goldenhar syndrome patients (Khong, Ophthalmology, 2013; Mansour, Am J Ophthalmol, 1985)
- Can also be associated with organoid nevus syndrome (Insler, Br J Ophthalmol, 1987; Diven, Arch Dermatol, 1987
Differential diagnosis
- Orbital fat prolapse
- Dermoid cyst
- Lacrimal gland prolapse
- Lacrimal gland cyst
- Lacrimal gland tumor
- Nonspecific orbital inflammation
- Conjunctival lymphangioma
- Conjunctival lymphoma
- Conjunctival squamous cell carcinoma
Patient management: treatment and follow-up
Natural history
- Dermolipomas grow slowly, and may become noticeable by teenage years
- Most, especially small and asymptomatic dermolipomas, do not require treatment and should be observed
- Surgery for this benign lesion should be avoided whenever possible, and, if pursued, should be minimal and meticulous
- Indications for consideration of surgery:
- Long-term intractable ocular discomfort
- Obstruction of the visual axis
- Induced astigmatism
- Cosmetically unacceptable in primary or medial gaze
- Patient must be fully informed of the potential complications before proceeding with surgery
Surgery
- Surgical debulking: If required, treatment involves debulking of the anterior visible portion only, through a conjunctival incision
- Complete excision is not usually recommended, due to potential deep extension of the mass around delicate orbital structures like the levator aponeurosis, lateral rectus, and lacrimal gland ductules
- Due to abnormal densely adherent conjunctival tissue, dissection around the dermolipoma can be challenging.
- As much healthy conjunctiva as possible should be preserved, while removing all pilosebaceous units and abnormal adherent conjunctiva.
- The conjunctival defect should be sutured via direct closure or with a rotational conjunctival flap or V-to-Y closure for larger defects (Choi, Br J Ophthalmol, 2015; Vahdani, Ophthal Plast Reconstr Surg, 2021)
- Histopathologic specimen examination confirms the diagnosis
- Intra-operative challenges: surgery may be more difficult than initially perceived due to the adherent nature of the conjunctiva with underlying tissue and proximity of surrounding orbital structures
- Occasionally no accessible dissection plane due to firm union between the tumor and conjunctiva
- Avoidance of dissection too close to the lacrimal gland, lateral rectus muscle, and levator/Müller’s muscle complex is key
- If necessary, a muscle hook can be used to identify the lateral rectus muscle
- Resection should be focused on functional and cosmetic improvement of the portion visualized in primary gaze
- Posteriorly, only portions anterior to the lateral orbital rim should be removed
- While the color and texture of the dermolipoma area may appear similar post-operatively, thickness will improve
- Removal of hidden portions of the mass is not essential and entirely dependent on ease and safety
Preventing and managing treatment complications
- Post-operative complications (Vahdani, Ophthal Plast Reconstr Surg, 2021):
- Persistent symptoms
- Shortage of conjunctiva
- Symblepharon to the lateral canthus
- Post-operative restrictive strabismus
- Injury to adjacent orbital structures:
- Dry eye due to damage of lacrimal gland ductules
- Ptosis due to damage of levator aponeurosis or from scarring
- Diplopia due to damage to or scarring involving the lateral rectus or conjunctival scarring preventing adduction of the globe
- Damage to the globe
- Orbital hemorrhage
Patient instructions
- Periodic monitoring for post-operative symptoms
- Post-operatively, the patient may still notice the lesion, but after debulking it should improve in thickness and appearance.
Disease-related complications
- Progressively enlarging dermolipomas may result in poor cosmesis, disturbance of vision via obstruction of the visual axis or induced astigmatism, and ocular irritation
- As choristomas, dermolipomas are normal tissue and, thus, do not harbor malignant potential
- The benign tumor may recur, however it is unclear whether recurrence is due to regrowth or herniation through a dehiscence in the fascia
Historical perspective
- Case reports of dermolipoma date back as far as 1854 (Kranka, Annales d’Oculistique, 1854)
- Sullivan (1972) and Beard (1990) inscribed warnings of the disastrous hazards of dermolipoma surgery using the old proverbs “Caveat Chirurgicus” (let the surgeon beware) and “An Ounce of Prevention Is Worth a Pound of Cure”
- Their experiences were fraught with numerous challenging and unrewarding subsequent surgeries carried out in efforts to ameliorate post-operative ptosis and diplopia
References and additional resources
- Kim E, Kim HJ, Kim YD, Woo KI, Lee H, Kim ST. Subconjunctival fat prolapse and dermolipoma of the orbit: differentiation on CT and MR imaging. AJNR Am J Neuroradiol. 2011;32(3):465-467. doi:10.3174/ajnr.A2313
- Shields CL, Shields JA. Conjunctival tumors in children. Curr Opin Ophthalmol. 2007;18(5):351-360. doi:10.1097/ICU.0b013e32823ecfbb
- Shields JA, Shields CL, Scartozzi R. Survey of 1264 patients with orbital tumors and simulating lesions: The 2002 Montgomery Lecture, part 1. Ophthalmology. 2004;111(5):997-1008. doi:10.1016/j.ophtha.2003.01.002
- Khong JJ, Hardy TG, McNab AA. Prevalence of Oculo-auriculo-vertebral Spectrum in Dermolipoma. Ophthalmology. 2013;120(8):1529-1532. doi:10.1016/j.ophtha.2013.01.015
- McNab AA, Wright JE, Caswell AG. Clinical features and surgical management of dermolipomas. Aust N Z J Ophthalmol. 1990;18(2):159-162. doi:10.1111/j.1442-9071.1990.tb00608.x
- Vahdani K, Rose GE. The Presentation and Surgical Treatment of Peribulbar Dermolipomas. Ophthalmic Plast Reconstr Surg. 2021;37(3):226-229. doi:10.1097/IOP.0000000000001848
- Mansour AM, Wang F, Henkind P, Goldberg R, Shprintzen R. Ocular findings in the facioauriculovertebral sequence (Goldenhar-Gorlin syndrome). Am J Ophthalmol. 1985;100(4):555-559. doi:10.1016/0002-9394(85)90681-6
- Insler MS, Davlin L. Ocular findings in linear sebaceous naevus syndrome. Br J Ophthalmol. 1987;71(4):268-272. doi:10.1136/bjo.71.4.268
- Diven DG, Solomon AR, McNeely MC, Font RL. Nevus sebaceus associated with major ophthalmologic abnormalities. Arch Dermatol. 1987;123(3):383-386.
- Choi YJ, Kim IH, Choi JH, et al. Early results of surgical management of conjunctival dermolipoma: partial excision and free conjunctival autograft. Br J Ophthalmol. 2015;99(8):1031-1036. doi:10.1136/bjophthalmol-2014-306328
- Kranka. Tumeur Lipomateuse de la conjunctive oculaire. Annales d’Oculistique. 1854; 31:105.
- Sullivan GL. Caveat chirurgicus. Trans Am Ophthalmol Soc. 1972;70:328-336.
- Beard C. Dermolipoma surgery, or, "an ounce of prevention is worth a pound of cure". Ophthalmic Plast Reconstr Surg. 1990;6(3):153-157. doi:10.1097/00002341-199009000-00001
Financial disclosures
Authors
Daniel Azzam: None
Seanna Grob: None